


About
There have been a number of recent efforts to build global maps of infection risk for different pathogens. These maps typically use the results of regressions in well-characterized settings to quantify the association between the presence of a pathogen and environmental, population density and climatic covariates as estimated through satellite data. These models are then used to predict the occurrence of the pathogen elsewhere. While a useful starting point, their ability to accurately describe the patterns of infection around the world remains unclear. It is largely unknown how representative the locations used to train the models are of places elsewhere. These models are not able to incorporate local differences in risk behaviours into their estimates leading to potentially misleading results.
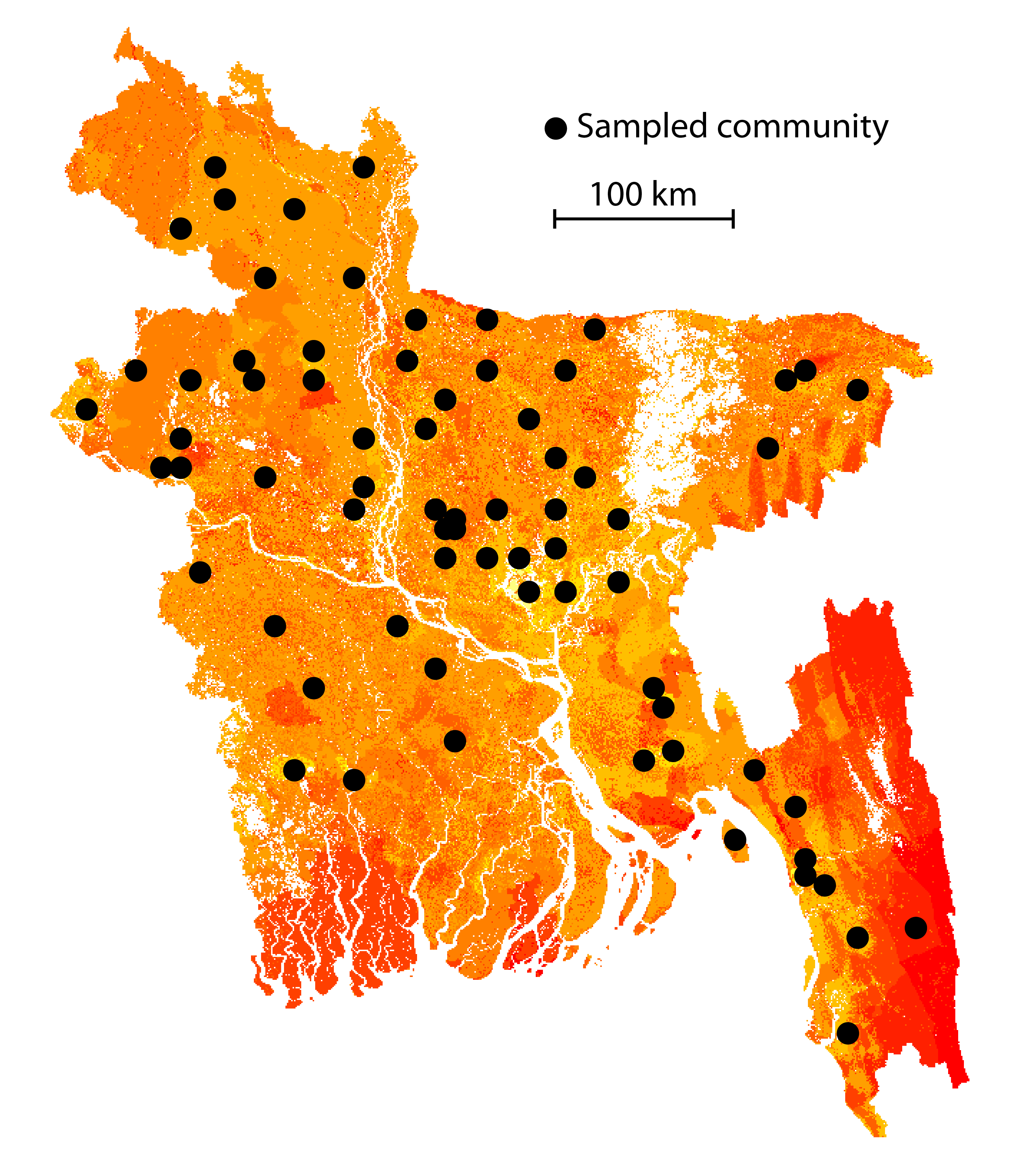
In partnership with the icddr,b (Emily Gurley), we are conducting a number of field studies in Bangladesh that are providing a more detailed understanding of arbovirus infection risk in a setting where arbovirus epidemiology is poorly understood. We are collecting data on human mobility patterns (as characterized through movement diaries, questionnaires and the wearing of GPS loggers for four days), trapping and identifying mosquitoes as well as collecting serum samples from individuals from throughout the country. About 16,000 serum samples collected as part of the studies have been tested for a panel of pathogen-specific antibodies including dengue, chikungunya, Japanese encephalitis, hepatitis E, cholera and Zika. We are using integrative mathematical models to explain the observed variations in observed seropositivity using individual behaviours, pathogen-specific characteristics and environmental attributes.
Similar analyses are being performed for arboviruses in French Guyana with Claude Flamand (Institut Pasteur Cayenne) and for influenza in Madagascar with Jean-Michel Heraud (Institut Pasteur Madagascar).