Link to Pubmed [PMID] – 24239323
Lancet Infect Dis 2014 Jan;14(1):50-56
BACKGROUND: The novel Middle East respiratory syndrome coronavirus (MERS-CoV) had, as of Aug 8, 2013, caused 111 virologically confirmed or probable human cases of infection worldwide. We analysed epidemiological and genetic data to assess the extent of human infection, the performance of case detection, and the transmission potential of MERS-CoV with and without control measures.
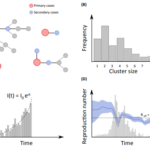
METHODS: We assembled a comprehensive database of all confirmed and probable cases from public sources and estimated the incubation period and generation time from case cluster data. Using data of numbers of visitors to the Middle East and their duration of stay, we estimated the number of symptomatic cases in the Middle East. We did independent analyses, looking at the growth in incident clusters, the growth in viral population, the reproduction number of cluster index cases, and cluster sizes to characterise the dynamical properties of the epidemic and the transmission scenario.
FINDINGS: The estimated number of symptomatic cases up to Aug 8, 2013, is 940 (95% CI 290-2200), indicating that at least 62% of human symptomatic cases have not been detected. We find that the case-fatality ratio of primary cases detected via routine surveillance (74%; 95% CI 49-91) is biased upwards because of detection bias; the case-fatality ratio of secondary cases was 20% (7-42). Detection of milder cases (or clinical management) seemed to have improved in recent months. Analysis of human clusters indicated that chains of transmission were not self-sustaining when infection control was implemented, but that R in the absence of controls was in the range 0·8-1·3. Three independent data sources provide evidence that R cannot be much above 1, with an upper bound of 1·2-1·5.
INTERPRETATION: By showing that a slowly growing epidemic is underway either in human beings or in an animal reservoir, quantification of uncertainty in transmissibility estimates, and provision of the first estimates of the scale of the epidemic and extent of case detection biases, we provide valuable information for more informed risk assessment.
FUNDING: Medical Research Council, Bill & Melinda Gates Foundation, EU FP7, and National Institute of General Medical Sciences.